
The Safe and Sound Protocol-Eighteen Months On
Heather MacDuffie, PhD, LCSW with Samar Singh, PhD, and Susi Lippuner, MSW
Background
This is a brief report about what providing the Protocol to approximately 80 individuals and sharing learning across the world about several hundred more has taught me so far.
Eighteen months ago, I learned about the Safe and Sound Protocol (SSP) as an intervention for the treatment of trauma and other self-regulation disorders. My experience working with traumatized clients for over 20 years led me to look for fresh ideas to improve my results. I was familiar with the Polyvagal Theory and the research of Stephen Porges, and certain that an intervention that he designed would be based on solid science and worth a look.
After taking the protocol myself, I felt convinced that this tool would take the world by storm. I did not at the time realize just how new the application of the SSP to clinical work with traumatized, anxious, and depressed individuals was. It has been used much more with individuals who have developmental disability, speech/language disorders, and autism. Which were Dr. Porges’ topics of focus when he first developed the SSP after developing the Polyvagal Theory. The SSP also has broader use in educational settings with children who have sensory and learning difficulties with great effect.
As a consequence and to my surprise, the decision to provide the SSP has involved extensive studying. The investment to work together and ‘give back’ is something I have never encountered before. Our work together has evolved to include an international collaboration with others including parents, teachers, providers, and researchers. What we share is a passion for the kinds of results that we see with the Safe and Sound Protocol. Many of us have a personal conviction about the SSP rooted in our own incredible experiences with the Protocol as well.
Results Overview
A word about evidence
When we evaluate an intervention, we can collect three basic kinds of information: That which can be measured by instrumentation, that which can be observed, and that which can be directly experienced and described. We find that with the SSP, all three types of evaluation are possible.
Measured Evidence
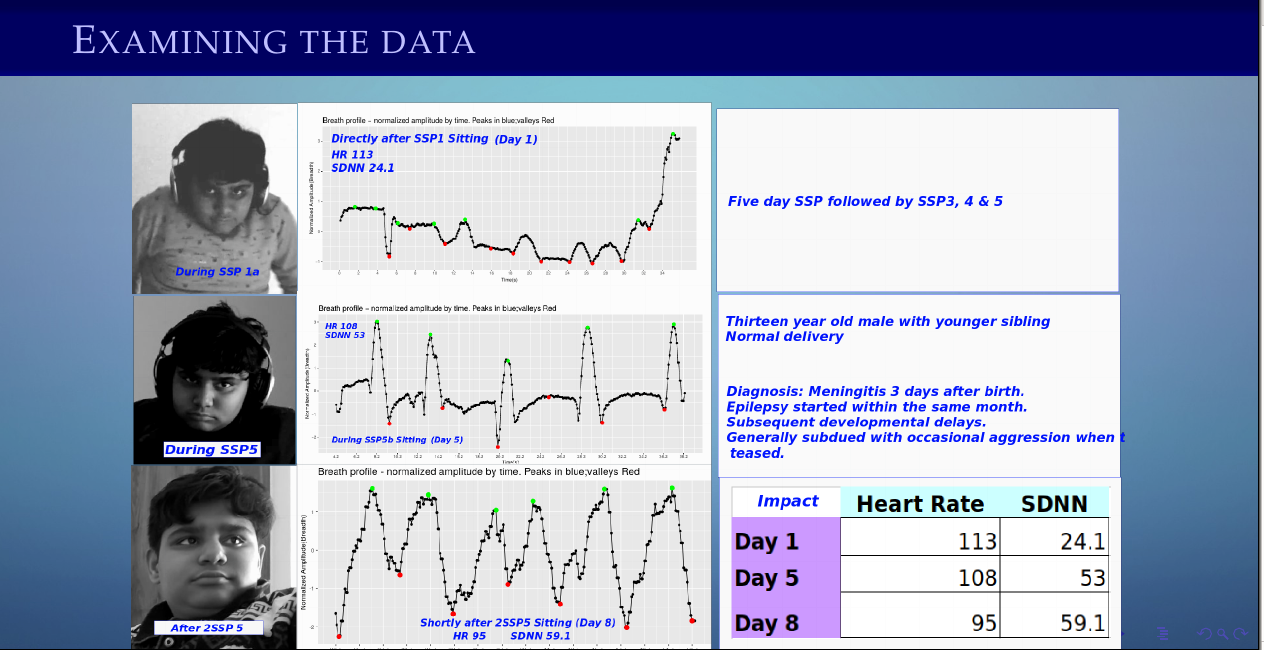
In our collective experience, taking the Protocol is correlated with broad-ranging changes in physical body states and behavior. As a group we have documented changes in heart rate, heart rate variability (HRV), and breathing patterns. After taking the Protocol these ‘bio-markers’ of our automatic/autonomic system (ANS) shift towards functional baselines that are seen with of healthy and stable functioning.
Healthy respiration when graphed has a regular s-shaped curve. Individuals who respond to the SSP demonstrate disrupted respiration patterns due to poor breathing patterns, including breath-holding, (as in the case of traumatized individuals) and upper chest breathing. Also, heart rate and rhythm is affected in ways that disrupt healthy functioning. Healthy variability in the heart rate is reduced. Reduced HRV is associated with numerous health problems, including cardiac arrhythmia. Completing the Protocol is associated with healthier breathing and heart patterns.
Here are two examples of breathing changes before and after listening to the SSP. Note the smoother peaked curves in the pink wave three months post-SSP in the first graph. Thanks to Samar Singh PhD for graciously providing these graphs of his work.

Respiratory pattern, before SSP, 3 months later. Samar Singh, PhD

Respiratory pattern, comparison of Days 1 and 4, SSP Samar Singh, PhD
The role of breath and heart rate in maintaining emotional state regulation has central importance in controlling state.
Observational Evidence
The number of responses that have been observed consequent to taking the SSP are extensive. A portion of the results that we have mapped collectively are included as the thumbnail for this blog post. Most prominent among them are increases in behaviors that involve the Social Engagement System and the ability of the individual to self-regulate. Self regulation opens the door to be able to respond differently to stress. As a psychotherapist, I appreciate how the SSP increases tolerance for engagement in the therapy process which accelerates therapy. Thus, in sessions I am explicit in mentioning increased tolerance for eye contact, more lively facial expression, voice tone and musicality, reciprocal interaction, and as well as increased spontaneous interaction. Clients are better able to put words to difficult emotions and less likely to dissociate, post SSP. They also have an increased ability to evaluate consequences accurately, are able to make decisions, activate and engage in flexible thinking.
With regard to hyper-activation or freeze symptoms such as are seen with PTSD, Social Anxiety, and Borderline Personality Disorder there is reduced reactivity in both directions, with fewer symptoms such as panic, disorganization, emotional reactivity, traumatic triggers, hypervigilance, hyperactivity, and a variety of other signs of chronic internal distress. Critically important is how chronic shame about being unable to control this, and emptiness related to chronic numbing and depressive states, alleviate.
Beyond psychotherapy there are other professional practice areas such as Speech/Language, Occupational Therapy and Education that have reported attention-getting gains. We see big gains in auditory processing, acquisition of speech and language, sensory integration, motor planning, reduction of sensory sensitivities and related behavioral meltdowns, and changes in bowel and toileting function.
So it is very clear, both in terms of markers of physiology and behavioral changes, that a global change in the state of the body and ease in the mind is elicited for many who listen to the SSP.
Social Engagement
The Safe and Sound Protocol works through improvements in the so-called Social Engagement System. When this system is activated, our physiological balance shifts to allow for calm, alert states: Those that are conducive to bonding, learning, digestion, and cell repair. What is this ‘system?’ It is an interconnected and coordinated array of muscles of the face, head and neck. Which work to generate expressions, voice tone, volume, and eye contact. These movements are coordinated in response to input from our eyes, ears, and other sense organs. They help us orient towards other beings in order to communicate our intentions.
Under flight/fight conditions, there are characteristic changes in our ability to control these factors, and in general there is a flattening and tension rises in the face and throat. One primary area of impact from the SSP is re-establishing calm states, softening facial tension, and establishing prosody in the voice. Numerous signs around the eyes and cheeks in particular indicate that facial nerve VII is being stimulated, as the features rearrange into a more focused and relaxed expression. It is quite remarkable to see the changes in facial expression from pre-to-post SSP.
Here is an example of the Social Engagement System ‘waking up’ during the administration of the SSP. The expression and gaze, as well as tension in the neck and shoulders have changed. Notice also the normalized respiratory pattern. Great thanks goes to Samar Singh, PhD, for graciously sharing these.
*Presented at Jacksonville Beach, Fl, at the iLs Gathering. April 25, 2019, by Samar Singh, PhD
Neural Exercise
Dr. Porges established that sound with certain qualities, rhythm, and tones can generate this state of calm alertness and provide an opportunity for positive interactions. Through engineered music, the Protocol elicits a ‘safe and sound’ state in the listener. This has also been called the ‘rest and digest’ state, as opposed to fight/flight, freeze or ‘fawn’ states. For lasting benefit, the individual must “exercise” by engaging socially while in calm states in order to lay down safe experiences of “being with” others. We know that this social calm has occurred when clients say that they can tolerate eye contact and focused interaction for the first time.
New learning is how we move beyond automatic reacting, thinking, and tensing due to uneasiness with others. For some who have experienced chronic fear or trauma, simply relaxing and feeling safe is actually frightening, and so they must first learn to tolerate experiences of the feeling of safety, before they are motivated to practice self-regulation. To be successful, therapy of any type must go beyond what can be accomplished with drills by recognizing the importance of someone being in a state in which they are able to learn. This is true because any therapy that involves an encounter with another being, and fearfulness when with others is the most essential component to address. As a psychotherapist, what I am often most interested in developing is an individual’s ability to engage with others as well as to allow me to help them encounter the compassionate truth of themselves in a calm way.
However (there’s always a caveat, isn’t there?), it’s important to emphasize that the states generated by the Protocol will very likely not remain unless the process of coming to calm alertness with the help of another is given practice through experience. Remember, we need practice with Social Engagement when the system has not functioned well for a while (if ever). Because each person has different interpersonal tolerances, different degrees of sensitivity to sensory data, (smells, sounds, lights, touch, flavor) and different levels of familiarity with their own senses (chronic numbing or dissociation, pain, and illness all affect this), there is no set protocol for “exercising.” Recommendations depend on a grounded assessment of what is happening now, and where to direct the next step.
Gaining insight into how best to connect each individual with the best “practice” support has been the steepest part of my learning curve as an SSP administrator. For example, someone who has a movement disorder in addition to self-regulation problems might benefit from the addition of physical therapy, reflex integration, or rhythmic movement work post SSP. Someone else might become involved with dance or massage. Or work on building reciprocal interaction and self regulation through play therapy. Depending on your existing treatment modalities and what has worked for you, recommendations for adjunctive therapies will require individualized consideration.
Reorganization and short term side effects
At times we see undesired ‘side effects’ in the weeks during and after taking the Protocol (up to 6 weeks, usually concentrated 2-4 weeks out). These may be reduced by ensuring that environments are welcoming, safe, and calm for starters. Side effects are considered mildly disruptive. Examples are: increased clumsiness, increased ringing in the ears, diarrhea, irritability, and explosiveness. Children who are aggressive may become more so. For these reasons it is helpful to know ahead of time as much about the current functioning of the individual with regard to self-regulation as possible, and to plan ahead to minimize additional sources of stress during this time. A full list of known short term effects is provided with the Protocol materials.
Because these undesired changes are short term and precede the onset of improved adaptive functioning I think of this as a reorganization period. Reorganization is a complex topic and beyond the scope of this blog. Briefly, if we are processing more sense data, learning more, relating to our bodies, senses and muscles differently. Then we will correspondingly adjust our reach, reset our balance, or question automatic thoughts. Adjusting takes time and practice, and is at times frustrating and uncomfortable. Our goal is to render it easier to adjust, be flexible and be resilient. In my experience, challenges are more likely to arise in children, whose dysregulation more often causes distress for others. Anticipating these issues and having other providers on board helps to reduce management problems and ensures that the Social Engagement exercise with skilled others will be part of the treatment period. The role of the family to support the changes the child goes through is critical to sustaining progress.